The Relationship with the Suffering Other. An Analysis of Attitudes Towards Respect for Older People in the Context of Social Services
Fabio Folgheraiter
Università Cattolica del Sacro Cuore, Milan
Maria Luisa Raineri
Università Cattolica del Sacro Cuore, Milan
CORRESPONDENCE:
Maria Luisa Raineri
e-mail: marialuisa.raineri@unicatt.it
Abstract
Population ageing, the increasing care needs of older people, shortcomings in Italian social policies, and the challenges posed by the pandemic some years ago have all highlighted a discrepancy between the widely proclaimed respect for the dignity of older manifests itself on structural, cultural, and even individual levels, including the attitudes of many social and health care professionals.
In this context, this study focuses three distinct positions, or ways of perceiving the respect for existential suffering, that may characterise the relationship between social and health care workers and older individuals: (a) the efficiency-oriented attitude (of neoliberal inspiration), in which respect and admiration are primarily directed at those who manage to age actively by «staying young» despite their age; (b) the «care-taking» attitude (of welfare orientation), which considers the elderly as deserving of respect out of professional duty, even when they are so ill or impaired as to be perceived as a burden to society; (c) the attitude of mature reciprocity (in a Relational sense), according to which it is the condition of suffering itself, that makes frail older people, worthy of being honoured by social services professionals, who approach them in a spirit of experiential learning. These three attitudes give rise to different types of care relationships, which will be analysed through the lens of the Relational paradigm. The empirical basis of this paper consists of a secondary analysis of qualitative data collected through 44 semi-structured interviews conducted during the pandemic (August-October 2020) in seven residential care homes in Emilia-Romagna, involving facility coordinators, care staff, family members, and elderly residents.
Keywords
Older people, Respect, Care relationship, Reciprocity, Social services.
Introduction
The principle of respect for other people, especially those in situations of vulnerability, is a historical cornerstone of the Codes of Ethics of the helping professions.1 A similar principle is also evoked in various ways in legislation and policy guidelines, beginning with Article 3 of the Italian Constitution.
However, as is often the case with principles of this kind, while it is easy to agree with them in theory, it is far more difficult to remain truly coherent when the issue confronts our daily lives and challenges the balance of competing interests. Moreover, the more the principle in question is considered self-evident, the more the adjustments and distortions that inevitably bend it to other aims tend to remain under the surface. This is particularly true for those working in the field — whether policy makers, service managers or frontline practitioners — since acknowledging oneself as «disrespectful» can be embarrassing and destabilising for one’s public or professional identity. For this reason, in the world of personal services, the dynamics of prejudice and discrimination are often subtle and unconscious, yet no less powerful in their effects (Strier & Binyamin, 2014).
Ageism (Butler, 1969; WHO, 2021) is a telling example. The ageing of the population and the growing health and care needs of older adults necessitate urgent strategies to make concrete the often-proclaimed respect to which all seem to subscribe. Yet the World Health Organization warns:
Ageism against older people is pervasive globally. It manifests itself in all key institutions in society. For example, in health and social care, where health care is sometimes rationed based on age; in the workplace during recruitment, employment and processes of retirement and dismissal; and in the media, where older people are often underrepresented. Globally, at least one in two people hold ageist attitudes towards older adults. Across the countries in the European Social Survey, one in three older people has experienced ageism. Thus, ageism affects billions of people globally (WHO, 2021, p. 37).
In this context of widespread yet under-addressed ageism, this contribution aims to support reflection, focusing particularly on social work practice, especially on the theme of inter-personal respect within the relationship between professional caregivers and suffering older adults. The central argument we propose is that certain ways of conceiving respect for older people, even when seemingly aligned with the ethical principles of social work, may conceal problematic assumptions. If not approached with awareness and critical sense, these assumptions hinder the development of a deeply respectful care relationship — one that endures even when the progression of decline appears to reduce the person to a mere body to be looked after.
Three Distinct Understandings of Respect
From our ongoing engagement with social workers and the organisations in which they are employed, we have developed the impression that, beneath the surface of language, three distinct attitudes — three modes or understandings of «feeling» old age and care — can be discerned in the field of personal services.
It is important to clarify at the outset that all three of these attitudes aim to combat ageism and seek to provide foundations for respecting older people. Each orientation has — as we will see — its own plausible rationale and thus cannot be labelled simply «right» or «wrong». However:
[...] there is respect and there is Respect. There is superficial respect, which glitters on the outside. And there is deep, radical respect. To respect and to Respect — paraphrasing Kierkegaard — are not the same thing. The two notions, although phonetically identical, may in practice clash on the semantic/emotional level: for instance, when a benefactor approaches a poor person with an air of superiority to offer «charity», they may outwardly convey respect while, deep down… not really (Folgheraiter, 2022).
As with all our convictions and sentiments, our ways of understanding respect are fundamentally rooted in culture and subsequently interwoven, in each individual’s experience, with personal psychological dynamics. Therefore, it is not surprising — and practitioners should not feel guilty — that these are predominantly implicit and unconscious attitudes, at least until a courageous act of reflexivity is undertaken. The culture of the society in which we live influences our ways of being like the current of a river carries swimmers downstream: without a conscious effort to swim against it, we will be dragged along, even if we believe we are in control of our direction (Thompson, 2021).
Within a first perspective, which we refer to as «efficiency-oriented», professionals reject ageism by asserting:
We social workers do not agree with the idea that older people are human waste, because although in our work we mostly see elderly people in severely compromised conditions, it is also true that there is a growing number of older individuals in good health who are active, engaged, informed, who travel, take care of their grandchildren, volunteer. They still live very well and have valid resources (both human and economic) — sometimes more than young people.
A second perspective adopted by professionals defends and respects the elderly on the basis of a broader concept that unites professional ethics with legal recognition of individual rights. We label this the «care-taking» orientation, which may be summarised as:
All elderly persons are fully human beings and must be treated as such, even those who are so ill or severely impaired that they objectively become a burden. A burden that is, nonetheless, still a human being and therefore has the right to be cared for.
A third type of respect, which we call «reciprocity-oriented», emerges from a sensitivity that is rarely articulated in professionals’ discourse and difficult to express explicitly. Nevertheless, it can be identified at the level of deep attitudes and emotional dispositions toward the suffering Other.
It represents a «tone» in how professionals relate to and perceive their «users» and the relationship with them. If one were to put this into words, it might be summarised as follows:
Precisely because you, the elderly user, are debilitated and confused, it is all the more evident that you are human. Precisely because you are now frail and in pain, you appear to my professional sensitivity to be a step ahead of me, existentially speaking. Your way of experiencing suffering, whatever it may be, offers a precious lesson through which I can grow in my own humanity.
To initiate a preliminary exploration of the empirical foundation of these three «attitudes», we conducted a secondary analysis of qualitative data originally collected for a different purpose (to examine the experience of the pandemic within residential care facilities) through 44 semi-structured interviews conducted between August and October 2020 in seven residential care homes for the elderly in the Emilia-Romagna region of Italy.
Interviewees included facility coordinators, frontline workers, family members, and elderly residents themselves (Corradini, 2021; for more details on context, participants, and data collection methods, see that publication).
Although our primary interest here is in the attitudes of frontline workers, we chose to analyse all interviews — including those with family members and elderly residents — based on the understanding that workers’ attitudes are not independent from those of their interlocutors: they both influence and are influenced by them.
The results of this analysis were then brought into dialogue with a preliminary exploration of the theoretical-analytical implications that we believe can be drawn from the ideas underlying the three ways of perceiving respect.
These were examined through the lens of relational analysis (Donati, 2013) and in light of professional ethics. The following sections will report on the data analysis and on the outcomes of these two lines of enquiry.
The Efficiency-Oriented Attitude (Neoliberal Orientation)
As is well known, discrimination is fuelled by negative stereotypes rooted in prejudices that generalise and flatten individual differences. Ageism is no exception. Therefore, in outlining the phenomenon to counter it, it is important to focus on culturally ingrained clichés that depict older people as inevitably weak, ill, mentally dull, naïve or temperamental (like children), lonely, and poor — in a word: lacking value. These negative stereotypes influence both individual behaviours and collective decisions, which translate into structural conditions of disadvantage, unequal treatment, or even oppression. At the same time, individual behaviours and structural disadvantages reinforce and confirm these stereotypes, creating a negative feedback loop that is difficult to dismantle (Thompson, 2021).
In this context, promoting an alternative representation of older people — supported by data on the growing potential for «active ageing» (Bramanti et al., 2016; Boccacin & Bramanti, 2014) — can be useful in dismantling prejudices. Indeed, it is undeniable that many older adults, whether due to genetic luck, personal merit, or the benefits of the welfare state, maintain a vitality typical of younger people, with all the objectively desirable consequences that come with it.
On the other hand, like all prejudices, ageist stereotypes also contain some basis in empirical observation: the very health and care advancements that enable many older adults to «stay young» also contribute to prolonging life into months or years marked by progressive decline, dependency, and suffering (Filippi, 2020; Fosti et al., 2024). Practitioners are well aware of this: many of their users are no longer «active» older people; indeed, most of them, to varying degrees, belong to this category.
Thus, while reminding ourselves that not all older people are a burden may help to deconstruct certain stereotypes, we must ask: is this really an adequate argument upon which to ground respect for older individuals? Before discussing this further, let us consider some examples.
Some Examples: I/You Am/Are Still «Doing Well», Despite Age
Older People Are Valuable If They Are (Still) Independent
In the interviews we analysed, many references were made to self-sufficiency as a primary value. The underlying idea is that people are appreciated and considered worthy of respect primarily because they are still «doing well», despite their age. Most notably, this perspective often comes directly from older adults themselves, who link satisfaction with their life to the ability to manage on their own.
For example, one woman explained, smiling, that she would prefer to die quickly rather than end up bedridden:
I’m quite happy, for someone who’s a hundred years old… and… I do everything by myself: I wash, I put on my diaper, I make my own bed… The caregiver tells me: we’ll do it for you! I say: no, I’ll do it myself!… So yes… I do it all on my own. Anyway, I always say: having come this far, never been bedridden for a day, I’m happy! Because my biggest fear is ending up in bed — that’s terrible for me. I always say: a quick stroke… Jesus has granted me many things… let’s hope He grants me this one too! (Resident A, 100 years old).
Another interviewee, though seemingly lucid, appeared to consider presenting herself as independent so vital to her identity that she insisted on it to the interviewer—despite not being asked, and despite it not reflecting her actual condition:
When I go to bed, I do the things I need to do, I manage myself, you know… I get dressed… in a way that… I do it better… (Interviewer’s note: a professional carer enters and, during a brief aside, tells me without being heard that the woman receives help for everything) (Resident B, 87 years old).
Another sign of how much value is attributed to self-sufficiency is seen in the reluctance of some to accept care («My mother has always been… let’s say… reluctant to let others take care of her», son F, 60 years old), as well as the willingness of residents to help out despite their limitations. Even a care worker recognises and appreciates this attitude:
There’s a resident who sweeps the floor for us after lunch, and whoever can help, helps gladly… especially older women who worked their whole lives, maybe in the fields… so they enjoy taking part in our work and helping us… it’s hard to serve them, you know — they always want to help, and that’s great (Care worker E, 40 years old, 8 years of work).
Not All Older People Are Fragile — or Not as Fragile as One Might Think
In line with this appreciation, even in a setting like a care home — where few residents appear youthful — we found traces of the idea that older people are more admirable the more they resist senile decline. For example:
In the end, older people are indeed fragile, but some of them — who seemed like they would die [from Covid] — are now pruning olive trees in the garden. It even happened that one of my care workers caught Covid, and so did her mother: the mother recovered very quickly, while the poor care worker took over two months to get better… (Head of care services G, 58 years old, 30 years of work).
A family member also expressed a view aligned with the efficiency-oriented sentiment. A passage from his interview highlights the dark side of valuing independence: when it is gone, the only «use» for older people is as consumers of care—and, thus, as a source of income for salaried caregivers:
Older people really are a burden on society… That’s how it is: they don’t produce anything, they cost money… My kids tell me: when I’m your age, I won’t have a pension like yours… you see what I mean? That’s where it starts… Sure, if you’re healthy, maybe you can help with your grandchild… some go to schools and help kids cross the street, I don’t know… some volunteer, but not all of them do: when you’re like my mom, in a care home… But hey! If there were no care homes, what would the people working there do? (Son D, 69 years old).
Discussion from the Perspective of Relational Analysis
The value of independence and health is so deeply rooted and widespread — at least in the Western cultural context — that it appears everywhere: in common expressions («health above all!»), in professional codes of ethics, for example:
The social worker […] promotes the autonomy of the person and […] enhances autonomy;2 […] enhances their autonomy, subjectivity and capacity to take responsibility,3
and in the principles of the main Italian law about social care:
The Republic... prevents, eliminates, or reduces conditions of disability, need, and individual and family hardship stemming from insufficient income, social difficulties, and lack of autonomy.4
The attitude that older people should be respected because some are just as vital as young people is at the foundation of liberal ethics, where the primary civic value is the possession of adequate energy/vitality to produce, enjoy, and consume. The ultimate good of the person lies in being self-sufficient — that is, being able to care for oneself and having a health status that allows this. Conversely, loss of independence must be prevented or, where possible, resolved.
The statistical assumption («many older adults today are still able, healthy, and enterprising») challenges the irrational ageist prejudice («everyone over seventy becomes a burden») and replaces it with a more inclusive principle: «All older people, even centenarians, are a resource as long as they are well and lucid». From this perspective, the ultimate reason to respect or even admire an older adult would be their vigour—their capacity to maintain the ideal condition of active ageing. Fortunately, we say, not all old people are... really old. According to this logic, an older person deserves respect and admiration because... they resemble a young person!
And the others? What about those who begin to need a carer’s help? Even more so: what about the «extreme elderly» — severely non self-sufficient, chronically dependent, confused, completely unable to move or speak, lying in bed awaiting death? When youthfulness is the value standard, we are led to reinterpret decline as merely pitiful. Severely impaired older people are no longer seen as persons but, at best, as bodies: biological mechanisms that have outlived themselves, in line with the chilling definition of senile dementia as «a death that leaves the body behind» (cited in Kitwood, 1997).
This is not to question the value of health and individual autonomy. These are indeed precious goods, pillars of life that we all have a duty to preserve — but they are not the highest goods. Above health and autonomy lies, quite simply, life itself. Most people, after all, live without being perfectly «healthy», whatever that may mean, and no one lives in a state of absolute individual autonomy. Rather, from a social work perspective, our human condition is characterised by interdependence (Folgheraiter, 2011).
In any case, health and autonomy should never be placed so high that they lead us to disparage their opposites: dependency, illness, degeneration, and death. Admiration for «healthy» and «active» older adults is certainly justified, as long as it does not result in contempt for its opposite. The principle that the autonomy of older people has to be promoted is entirely valid, but it is not a sufficiently solid foundation on which to base the respect for them.
The Components of a Care Relationship Oriented Towards Efficiency, According to the AGIL Scheme
To further explore the implications of this line of reasoning, let us attempt to analytically identify the components of the care relationship between care workers and elderly persons that might emerge from an exclusively efficiency-oriented approach — bearing in mind, of course, that in the actual flow of relationships, the ways in which respect is experienced are always intertwined in specific contingent configurations, which vary from one relationship to another and over time.
We follow (Figure 1) the AGIL scheme (Donati, 2013), beginning with the value system (L), which in this case foregrounds efficiency, health, productivity, and individual autonomy. In the context of helping relationships and care policies, this value horizon is linked to a set of objectives (G) that can be summarised under the label of «active ageing»:5 the goal is to ensure that older persons maintain, as much as possible, a life that is physically and mentally similar to that of adults or even of the young. The means (A) for achieving these objectives consist of prevention and activation programmes which, precisely, constitute the policies for active ageing. The behavioural norms (I) that regulate interaction consist primarily in the idea that older persons have a duty to remain as healthy and autonomous as possible, by diligently following the guidance of experts in order to «stay young», so as not to become a burden to others and to society (even before being a burden to themselves…). Symmetrically, experts are expected to provide such guidance.
In summary, a sense of respect towards the elderly that is framed in efficiency-oriented terms appears to be problematically linked to a care relationship that is «exclusively» preventive in nature: both professionals and older persons believe that the ideal would be not so much to prevent ageing itself (since time cannot be stopped), but rather to slow down its effects (secondary prevention) and reduce its negative collateral consequences (tertiary prevention), including repairing, where possible, the dysfunctions that progressively emerge. If this is not possible, there is nothing left but to regret the lost health.
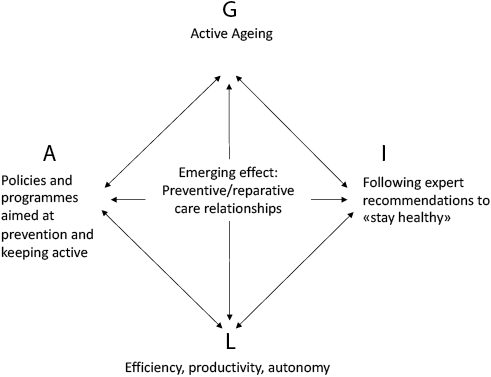
Fig. 1 Components of the efficiency-oriented care relationship.
The «Care-Taking» Attitude (Welfarist Orientation)
The second way of conceiving respect for older people is likely the most deeply rooted within the culture of social and healthcare services. Professionals oriented in this way do not consider their user less deserving of respect — almost as if they were a second-class human being — simply because they are no longer efficient or healthy.
Alongside the duty to promote personal autonomy, these practitioners remain acutely aware of the principle that no person should ever be treated as disposable, even when it may be difficult to deny that, objectively, «they are so».
This attitude can be expressed as follows: «You have irreversibly become a burden to society, but we, as professionals, will never refuse to carry out our job, which is, in essence, to carry you on our shoulders».
In place of the earlier efficiency-oriented attitude, two considerably more nuanced guidelines are adopted here: one is deontological («our moral duty as helping professionals requires us not to disdain our users’ weakness»), the other legal («however civically diminished some of our users may appear, they remain full rights-holders»).
Some Examples: I Respect You Because You Have the Right to Be Respected, Despite Your Decline
Care-Taking Is a Duty, Regardless of the Person’s Condition
The idea that it is a duty to respect and care for frail and suffering older people —even if it is a one-sided act of «giving» — was nearly unanimously present in the interviews we analysed.
As expected, professionals primarily invoke duty as a professional obligation that remains binding even when they are fully aware that this is, in a sense, a «losing» endeavour, as there is no future ahead. For example:
We are part of... the third phase of their lives. Let’s be clear... there is nothing after this. But we still have the duty to give them quality (Coordinator D., 42 years old, 10 years of work).
What kind of life do we want to offer these older people? Do we want to relegate them to the bottom of the barrel? My job is to treat them not based on age or life expectancy but based on what they are still able to experience. Let’s help them live this stage in the best way possible. (Head of care activities C., 43 years old, 7 years of work).
With a grandfather suffering from a severe condition, like advanced dementia, it’s more complicated... But in the end, they must always be treated the same way, in my opinion. They must always be treated well, to help them feel as well as their condition allows. I mean… in our work, helping them feel well must always be the top priority, the way I see it. (Care worker 2D., 44 years old, 1 year of work).
Similar views were expressed by several family members of older residents, often invoking a broader moral duty.
In these statements, the underlying idea remains that the decay associated with ageing holds no intrinsic value; the motivations for treating older people with respect lie in our sense of civilisation and human compassion:
Weak people who need extra attention are a problem? So, what do we do? Bring back the guillotine and eliminate them? (Son F., 60 years old).
Daughter-in-law of a resident: «If someone is old and in bad shape… should we just let them die? A little humanity, please!». Husband of the same resident: «I believe there are elderly people in there who have no relatives and are always alone... where should we put them? Under a bridge?» (Husband D., 82 years old).
Some interviewees even seemed to suggest that the idea that ageing diminishes human «quality» is so deeply ingrained that signs to the contrary are perceived as exceptional. For example:
«I... love my mother very, very much, despite the fact that she’s 91…» (Daughter B., 65 years old)
«You know, they see, they hear — it’s not like they’re dead: they’re alive, even if they can’t speak, they can still sense the atmosphere…» (Care worker 2B., 58 years old, 12 years of work).
Care-Taking as a Duty to Repay What Older People Have Done: Reciprocity Ex Post
A variation of the care-taking attitude consists in grounding it — and respect for the elderly — in the duty to repay the contribution they made during their earlier lives. This is a form of symbolic exchange (Rossi, 1989; Bramanti, 2001; Donati, 2007), in which we care for older people out of gratitude for what they once did. Once again, no value is attributed to what they are now; rather, the appreciation is retrospective. Gratitude is certainly a commendable sentiment, but it does not challenge the idea that a severely impaired older person matters only for who they were, not for who they are.
We found many examples of this attitude in interviews with both professionals and family members. As expected, the latter — especially children or grandchildren — often refer to a «situated» sense of gratitude, specifically tied to their past relationship with the loved one:
She [my mother] felt guilty and we explained to her several times: «Mom, when we were little, you gave your time to us. Now that you are the one in need, we’re giving you back the time you gave us, and we do it gladly» (Son D., 69 years old).
When I was a child, my grandmother used to take me to kindergarten, she watched me play in this very same garden, and now… I feel like it’s my turn to return the favour by coming here… (Granddaughter B., 38 years old).
Professionals, on the other hand, tend to speak more generically about the contribution these elderly people (presumably) made to others or to society during their earlier lives:
If you exist, it’s because this grandmother brought your father or mother into the world, and they gave you life. So, if she made sacrifices for them, why shouldn’t you make some sacrifices for her? Besides, these elderly people are at the end of their lives — it’s not like you’ll have to care for them forever… (Care worker 2B., 58 years old, 12 years of work).
It’s part of the life cycle: before being old, they were young, and they cared for others… (Coordinator A., 39 years old).
Care-Taking as a Duty Because «Someday It Will Be Our Turn»: Reciprocity Ex Ante
A third variation of respect despite decline mirrors the one just described: we consider care-taking a duty today as a way to affirm a principle that may apply to our own future lives, when we — whether as professionals or family caregivers — will become fragile and «useless» older people ourselves. This is a form of anticipatory reciprocity, as if we were symbolically accumulating credits for the future. Here are some examples of this widespread attitude:
People get old! I always tell myself this: when it’s my turn, I hope there will be someone by my side who… will look after me. Turning these people into a problem… for me, that’s wrong! (Son F., 60 years old).
What does it even mean that the old weigh on the young? That young person will (hopefully) also grow old and weigh on someone else… It’s a chain: we are born children, we become adults, we grow old… (Care worker 2D., 44 years old, 1 year of work).
I found it horrible, this feeling of relief some people had about Covid was killing more the elderly that the young people... We’ll become old too — maybe! (Coordinator B., 41 years old, 10 years of work).
It is worth noting that imagining oneself in the shoes of today’s elderly users or relatives is neither easy nor spontaneous. There is an emotional difficulty in facing the suffering that may await us — and the death that will certainly come — and this is reinforced by the efficiency-oriented culture, which, as previously noted, makes the loss of autonomy and health seem even more tragic and tends to suppress the very notion of death (Ariès, 1978). Yet, the ability to imagine oneself as old and in need is a fundamental premise for the Golden Rule of universal ethics («Do unto others as you would have them do unto you»), which is also a foundational principle of social work (Folgheraiter, 2014). The deep and immediate respect that a professional or family caregiver attributes to themselves can then be transferred — by analogy — to the frail person in their care. Thus, attitudes guided by ex ante reciprocity are certainly commendable. However, as expressed in our interviews and in common discourse, they too have a dark side: they do not challenge the idea that, at a certain point, both the older people we care for today and we ourselves — someday — will be actual cast-offs, of no value. Hopefully, we may still reach the end of life with some dignity, thanks to the goodwill of our caregivers and the welfare system.
Discussion from the Perspective of Relational Analysis
The position that frail older people have a right to be respected, despite their decline, is a necessarily reaffirmed truism and forms the foundation of welfare state ethics and every constitutional mandate: the right to care and respect must be guaranteed to all by authority, without exception — whether to non-self-sufficient older people or to any other form of biological or behavioural «deviance». This principle is also indispensable to the helping professions, which might otherwise lack any raison d’être outside of this ethical and political framework.
However, the undeniable value of this perspective does not mean that it represents the best possible foundation upon which to anchor respect for the suffering Other. In fact, one could derive the following slippery conclusion: that older people are not to be respected intrinsically — that is, «in themselves», for the value they hold here and now. Rather, they should be considered worthy of respect for what they have been, namely, for what they did during their previous, active lives — the only phase that, in the eyes of professionals and perhaps family caregivers, still retains any value.
The logical corollary of this reasoning — equally problematic — is that the respect due to these severely deteriorated, confused, almost ex-human elders must come from a one-way dedication sanctioned by the welfare system and embodied by care professionals. As if to say: in our enlightened age, these poor cast-offs are fortunate to find us, the helping professionals — skilled and civilised — who do not withhold any rights from them, despite their now irreversibly diminished condition.
A rights-based theory — while correct and necessary in its abstract formulations — does not always translate into deep respect when «personalised», that is, when applied to a specific individual. Thinking Even though you are now, in every way, a burden, you can count on me expresses a noble intention in the abstract, that risks contradicting itself in practice.
To implement such an intention inherently implies a stance of superiority: it is only due to our goodness, humanity, or civic duty that we care for this specific Other, who here and now no longer holds any value. Thus, a trace of benevolent contempt underlies our very words of praise and acts of care.
In emphasising the weakness of our interlocutor, we socially consolidate it. We end up thanking God that we are (still) not like them — thereby becoming unconsciously self-righteous.
Components of the Care-Taking-Oriented Care Relationship According to the AGIL Scheme
The components of a care relationship grounded in the care-taking attitude (see Figure 2) include a value system (L) centred on the right to assistance and the civic value of treating even the weakest with humanity and respect — with possible drifts toward paternalism and excessive benevolence. The situated goals (G) pursued to translate these values into practice consist precisely in «taking on care», i.e., supporting those who cannot support themselves, by stepping in for them in the many (or all) areas where they are no longer able to act. The means (A) for implementing care-taking include personal care services: home assistance, supported housing, long-term care facilities, and the many varied forms of social and health support provided in such settings. To these, we may also add monetary benefits such as attendance allowances — crucial for paying private carers — or care grants that help support the efforts of family caregivers. The behavioural expectations (I) that govern this type of care relationship revolve around the idea that the non-self-sufficient older person should trust and accept care, while professionals and family caregivers assume the duty of providing it. In summary, a notion of respect for older people based on rights is linked to a care relationship that is essentially assistive or palliative in nature: respect is due even when individual conditions have declined to such an extent that there is nothing more to prevent or repair. The only path left is to substitute ourselves to the impaired person, meeting their basic needs and any other needs they are still able to express — while waiting for life to end. In such a care relationship, direct reciprocity is not contemplated: the roles of helper and helped are dichotomous, since it is assumed that the severely impaired older person has nothing left to give. In their here and now, they are worth nothing.
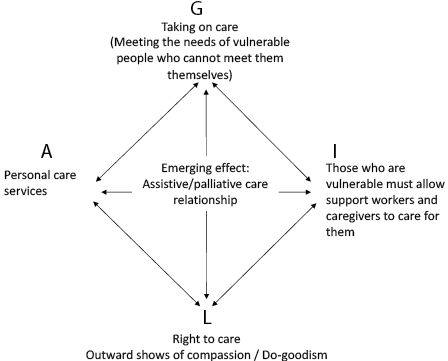
Fig. 2 The components of the care-taking oriented care relationship.
The Attitude of Mature Reciprocity (Relational Orientation)
The third posture consists in approaching the pain and decline of the person by also, and above all, recognising the humanity inherent in such suffering. Even when certain older adults appear outwardly as societal outcasts, they are perceived by the professional or informal carer as fully human — precisely because of their impairments and limitations—which render them examples of life itself, to such an extent that the relationship with them may enhance the carer’s own humanity and professionalism.
Respect, understood in a relational sense, incorporates the «virtues» of the second attitude, while also cleansing it of the dark side previously discussed. It presupposes, even within a professional context, a tendency toward human equality in the relationship between the carer and the cared person — beyond professional or social obligation and compliance with external regulatory norms. It is on this equality that a deeper respect for the suffering Other is founded.
In such a care relationship, care worker or informal carer perceives themselves as being on the same level as the person they assist, first and foremost (a) in the sense that both share the human condition, and with it, the potential to experience — in the full sense — illness and suffering. But they are also on the same level because (b) each brings value to the other. The carer is not there, in the relationship, solely to «give» (physical care, compassion, emotional closeness, and so on), as should be self-evident, but also to receive, in terms of humanity: the way the suffering Other lives their decline and pain — whatever that way may be — constitutes, in the here and now, a valuable life lesson, as well as a professional one.
In proximity to the suffering Other, in a respectful and affectionate relationship, the carer may «receive the gift» of a vicarious experience of conditions they have likely never endured, and perhaps never will.
Within this framework, then, respect is based on the intrinsic value, here and now, of the suffering Other. Clearly, this is not intended to romanticise the «beauty» of being ill, disabled, or cognitively impaired. Given the choice, no one would wish to be in such a condition — and rightly so — and it remains a professional obligation to intervene in support of well-being, so long as one does not cross into the controversial territory of overtreatment.
The reflection being proposed is another: the person who experiences the painful condition of senile decline — precisely by inhabiting an extreme state that is nevertheless intrinsically human — can take on inestimable value in the eyes of those who accompany them.
To attempt to clarify what this means in practical terms, we may imagine a carer connected to such a sentiment being guided, as they work, by an inner voice of wisdom that helps them implicitly convey to the person in their care fragments of a message such as the following:
Precisely because you now feel humiliated, as if discarded, you have value in my eyes.
The more you are experiencing pain or degradation that I have not yet known, the more you are, to me — and potentially to all of society — a teacher of humanity.
I am honoured to be able to assist you as a professional, and I thank you for your generosity in receiving me as I am. Even when your anguish overwhelms you and you experience my care as an intrusion, you — willingly or not — accept me. Thank you for allowing me to be by your side and to witness your life: in doing so, I will learn (Folgheraiter, 2022).
Respect understood in this way lies far from common sense and the cultural expressions we are used to, and is therefore difficult to express fully in words. Rather, it is intuited in the attitudes of those practitioners (and also of some family caregivers) who are radiant, harmonious, and broadly content with themselves and their work — who bear witness to the luminous power of a life more deeply understood, even at a time when, for lack of serious experience, it typically appears to others as a taken-for-granted daily routine.
Some Examples: I Respect You Because Your Humanity Is My Teacher
As one might expect, we did not find fully articulated reasoning of this kind in the interviews. However, traces of such a sentiment are detectable in several excerpts that suggest a process of learning — or personal growth — on the part of the caregiver, thanks to the person being cared for. For instance, the following respondents indicated that their relationship with older people offered them examples of courage in facing adversity:
[Facing the pandemic] was really difficult, but they [the elderly residents in the facility] gave us great strength… the strength to keep going always… it was truly them who gave us the strength to carry on in this difficult, emergency moment (Head of care activities F., 38 years old, 4 years of work).
They are people who, no matter how bad their condition is, never die: they’re made of something else, physically and mentally... [my mother] has a kind of acceptance of her fate, a resilience... (Son D., 69 years old).
I have to say the residents were wonderful, and they taught us so much, because… what came out of all this? They immediately remembered the war and the post-war period — now they feel like they’re living through another post-war era... (Coordinator D., 42 years old, 10 years of work).
Others spoke of learning by being in relationship with their service users «there’s always something to learn in this environment, in this difficult world: it’s not for everyone, but it’s beautiful»; Care worker 2D., 44 years old, 1 year of work) and gaining first-hand experience that suffering and death are part of life (I had to learn this too… not everyone can be saved»; care worker E., 40 years old, 8 years of work).
Still others referred to the emotional quality that the relationship with older people — even those who are severely impaired — adds to the lives of carers and their loved ones, a quality that is felt even more strongly when someone dies unexpectedly, as tragically happened during the pandemic:
The hardest part was seeing residents die like that, because I’ve been here five years and so you build a bond… and suddenly you’d find yourself like that... with one less friend (Care worker F., 31 years old, 5 years of work).
Each one of them gives you something, from the centenarian I’d known for twenty years to the person with cognitive impairment who passed away — she was probably the last person I thought I would miss… but those were heavy losses. Even now, I sometimes look at their photos, because I’ve kept them with me (Head of care activities E., 48 years old, 10 years of work).
Each resident has their special person — the one they look for… I don’t know, that care worker… they can’t wait for them to come on shift… it’s a beautiful thing (Head of care activities F., 38 years old, 4 years of work).
I saw — really unexpectedly — older people who were better than any of us at giving that extra value [to the video calls during lockdown]... I can’t even explain it, because really… it has to be experienced (Coordinator D., 42 years old, 10 years of work).
The emotional value of the relationship in the here and now is also acknowledged by family members — even, and especially, when their loved one’s condition is very severe:
They gave me no hope, and yet [my mother] was still there. I wanted to enjoy her right to the very end — one hundred percent, really: every second (Daughter 1G., 49 years old).
She no longer knows I’m her daughter, but when she sees me, I’m someone she... well… she manages to connect with. I say ‘connect’ in a manner of speaking… she has trouble speaking, but she smiles at me. And so I’m very happy with that smile (Daughter E., 60 years old).
One specific expression of reciprocity emerges from the mutual help experiences shared by some of the elderly residents in care homes. To appreciate their significance, it is worth noting that these individuals have serious health limitations, reduced personal autonomy, and some level of cognitive decline.
Resident A: We helped each other during lockdown. All of us — even the residents. We play cards, we have fun, we laugh at silly things. We’ve created a nice little group. We help one another — if he needs something, I can support him morally, and she can too, and so can I... — Resident B: You have to be patient with everyone. — Resident C: You go and see how they’re doing... — Resident D: And you smile at everyone (Group of residents, aged between 85 and 74).
What helped me? Oh well… my roommate, my friend… sometimes we say something silly and laugh… and we made it through (Resident 5G., 85 years old).
These individuals express mutual appreciation and respect for one another as they are now, and some also honour their relationship with others who are no longer even partially self-aware — such as this resident who speaks of her sister, suffering from advanced dementia and living in the same facility:
How can I put it… we keep each other company, in the sense that I have a point of reference here, a family reference, and she has a presence… only a presence, because I can do very little for her, almost nothing... (Resident 1A., 85 years old).
A final excerpt is particularly interesting because, by contrast, it hints at the importance of a reciprocal relationship. The care worker is describing how their daily professional experience changed during the pandemic, when the sudden and overwhelming workload led them to treat service users more like bodies to maintain:
We weren’t caregivers — we were forklifts. «You have to do this and that»: no one even asked why, you were just there in the middle of it and you did it. [And even now] it’s not like it was before… you lift them, move them, feed them… but there’s no connection anymore... now they’re, how can I say... they’re alone. Closed in on themselves... Now sometimes I find myself becoming a machine — I no longer feel like the person I used to be. There are times when I ask myself, «What am I doing?»... I’m even starting to question whether it’s right to continue like this, or if it would be better to find another path — because I feel like I’m no longer truly helping (Care worker F., 31 years old, 5 years of work).
Discussion from the Perspective of Relational Analysis
The third way of perceiving respect is based on the lived experience of the principle of reciprocity: the premise for granting deep dignity to the fragile person — or the one degraded by decline — lies in perceiving that it is precisely their condition that can offer us a lesson. In «extreme» situations, when social and health care techniques and common sense suggest that there is «nothing more to be done», help and assistance can only reverse, so to speak, their polarity: we can no longer «give», in the strict sense of the word. We can only give by opening ourselves to reception — that is, by receiving. Donati writes:
The dignity of the elderly does not lie in what they have done, however great their contribution to society may have been. Nor does it lie in what they can still do in terms of useful things, like helping grandchildren and great-grandchildren. It lies in what the elderly person is in their humanity, which is given in their relationships — the simplest ones — even when confined to a wheelchair or suffering from a serious illness. Even when they are just a silent presence. Because even in these situations, what the elderly person can offer is the request for a human relationship that makes human the one who provides care. The quality of the care given by the caregiver is an act of reciprocity toward this dignity of the elderly (Donati, 2022, pp. 329-330).
We can only «transmit» respect to our interlocutor by allowing them to offer us teachings. These teachings may pertain to the practitioner’s professionalism, since that care relationship — if approached with adequate reflexivity — is a precious source of experiential learning to better understand how to work near death.
Moreover, a care relationship grounded in reciprocity offers significant existential value: the vicarious experience of suffering casts new light on life itself. It may prompt the carer — even now, while still healthy and autonomous — to feel health and strength as precarious and therefore precious gifts, far from being taken for granted.
If this attitude were genuinely internalised by practitioners and informal carers and gradually passed through networks of meaningful relationships, then we might imagine that the lessons learned from the experience of suffering and death could also yield social benefits. Those who carry out a helping profession with the mandate of accompanying others toward death — on behalf of us busy citizens and consumers —might still bring to our attention a testimony of what those people could have «told us», if only there had been the opportunity.
The principle of reciprocity has fundamental implications for all relationships. If we limit our focus to the field of social work and helping relationships, it is central to the ethics of care (Sevenhuijsen, 2003; Barnes & Brannelly, 2015), according to which care that does not recognise the intrinsic human value of suffering — and treats the Other as a body — is not care.
It is the basis of Relational Social Work (Folgheraiter, 2024), which teaches the practitioner to relate to every interlocutor by always seeing value in them. It is also the cornerstone of anti-oppressive approaches in contemporary social work (Krumer-Nevo, 2020; Fook, 2016), which expose and challenge the suppression of rights and power among those on the margins of society.
Components of the Reciprocity-Oriented Care Relationship According to the AGIL Scheme
The reciprocity-oriented care relationship (see Figure 3) is grounded in the recognition (L) of the intrinsic human value of experiences of suffering, decline, or marginalisation, and of those who bear them. This value horizon is connected to the methodological-professional goal (G) of co-constructing helping processes: if, as social workers, we are able to appreciate those we are called to assist, it would be inconsistent not to foreground their contribution in defining the goals to be pursued — whatever those may be.
The means (A) to achieve this involvement correspond to techniques of relational facilitation/guidance, which all share the trait of «working» only under certain conditions (I), the most important of which is the attribution of an overarching equal status between the helper and the helped.
The distinctive feature of reciprocity that emerges from this type of care relationship lies in the fact that the relationship enhances the human dignity of both parties: the person who provides care and the suffering person who receives it.
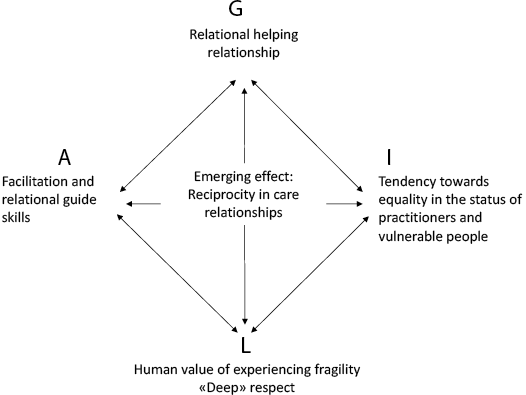
Fig. 3 The components of the reciprocity-oriented care relationship.
Conclusion
This discussion has led us to identify the ideal-typical features of three ways in which respect for the suffering Other may be conceived — or more simply, experienced. The first two, one anchored in the value of efficiency and individual autonomy, the other in the right to care, have a dark side: while one may affirm respect for the person, one simultaneously and unintentionally ends up devaluing them. The third, based on the principle of reciprocity, does not negate the previous two but goes beyond them, highlighting the human value to be recognised in fragile individuals, who are worthy of being honoured, here and now, precisely in their human fragility.
The exploratory analysis of a set of interviews with care professionals, family members, and elderly residents in residential facilities seems to confirm the presence, in the statements made by the sample, of all three forms of respect, although the third is articulated less explicitly — undoubtedly because it is much less deeply rooted at a socio-cultural level.
Respect for the Other is, by logical necessity, situated within a relationship, the components of which have been examined using the AGIL framework. The analysis has suggested that these components take on different configurations depending on how respect is understood and experienced.
The different types of care relationships that emerge in the three cases have significant implications not only for the user but also for the practitioner. This point, highlighted by relational analysis, deserves emphasis, given that most practitioners, relying on common sense, likely conceive of respect for service users as an attitude that must be assumed in the primary interest of the service users themselves. On the contrary: the dignity recognised in older people reflects the dignity of the professionals. The way practitioners experience respect toward their elderly users is mirrored in the respect and satisfaction they feel toward their work and, ultimately, toward themselves.
If the care relationship is centred on prevention and/or repair — as understood in terms of secondary or tertiary prevention — what happens when the possibilities for prevention and repair reach zero (as they inevitably do, since eternal life is not of this world)? If, in the implicit perception of practitioners, the most «prestigious» or truly legitimate care relationship is one in which suffering is mitigated or resolved, then when this is no longer possible, they may feel like second-class professionals, caring for people for whom, alas, «there is nothing more to be done». From the efficiency-oriented perspective, doing anything other than preventing or repairing is effectively doing... nothing—or at least, doing something of no value.
This underlying belief is widespread in the world of social services: from the self-perceptions of practitioners to the job preferences of new graduates (Weiss et al., 2002), to political decisions regarding, for example, the level of qualifications required to work with older people compared to those required to work with children.
When one identifies with a care relationship centred on caretaking, the strong ideal commitment to the notion that care is a right — despite the decline of old age —may protect one from feeling like a less skilled or less important professional. However, it does not shield one from the risk of burnout (Bellotti & Madera, 2008; Benini & Magenti, 2021), which is linked to a one-sided caregiving relationship in which the practitioner sees themselves as being called only to give and give, without receiving anything in return on a human level. They receive a salary, of course, but that is not enough to protect against the emotional exhaustion that results from constant contact with suffering and degradation that lacks meaning.
A reciprocal relationship, by contrast, calls the practitioner to pursue the good of the Other — in our case, the higher good of respect for human dignity — while seeking to uncover the potential for growth that stems from enabling the Other to offer something in return. In other words, it is a matter of pursuing the good of the Other in the awareness that it can only be realised by also increasing one’s own good.
References
ANEP — Associazione Nazionale Educatori Professionali (2015). Codice deontologico dell’Educatore professionale.
Ariès, P. (1978-2013). Storia della morte in Occidente. BUR.
Barnes, M., & Brannelly, T. (Eds.). (2015). Ethics of care: Critical advances in international perspective. Policy Press.
Bellotti, G. G., & Madera, M. R. (2008). Il burnout degli operatori geriatrici: Equilibrio e discordanza tra persona e lavoro. Ricerche di Psicologia, 1-2, 229-238.
Benini, S., & Magenti, N. (2021). Quando l’assistenza «nutre» e quando «svuota». L’esperienza di cura raccontata da un gruppo di infermieri. Medical Humanities & Medicina Narrativa, 19, 109-132.
Boccacin, L., & Bramanti, D. (2014). Anziani attivi in Europa tra morfogenesi dei legami e innovazione esistenziale. Studi di Sociologia, 3, 233-259.
Bramanti, D. (2001). La cura come forma del dono in famiglia. In G. Rossi (Ed.), Lezioni di sociologia della famiglia (pp. 167-190). Carocci.
Bramanti, D., Meda, S. G., & Rossi, G. (2016). Invecchiare attivamente tra le generazioni: Verso una società age friendly? In G. Rossi, & E. Scabini (Eds.), L’allungamento della vita. Una risorsa per la famiglia, un’opportunità per la società (pp. 3-44). Vita e Pensiero.
Butler, R. N. (1969). Age-ism: Another form of bigotry. The Gerontologist, 9(4), 243-246.
CNOAS — Consiglio Nazionale dell’Ordine degli assistenti Sociali (2020). Codice Deontologico dell’Assistente Sociale.
Corradini, F. (Ed.). (2021). La vita (e la morte) nelle strutture per anziani durante la pandemia. Una ricerca qualitativa in Emilia-Romagna. Erickson.
Dominelli, L. (2002). Anti-oppressive social work theory and practice. Palgrave Macmillan.
Donati, P. (2007). Capitale sociale, reti associazionali e beni relazionali. Impresa sociale, 2(76), 168-191.
Donati, P. (2022). Relazioni fra umani e relazioni fra umani e robot: Il caso dell’assistenza agli anziani. In P. Donati (Ed.), La teoria relazionale nelle scienze sociali: sviluppi e prospettive (pp. 313-346). Il Mulino.
Donati, P. (2013). Sociologia della relazione. Il Mulino.
Filippi, V. (2020). Più longevi ma con meno salute? Un allarme epidemiologico, I luoghi della cura, 3. https://www.luoghicura.it/dati-e-tendenze/2020/07/piu-longevi-ma-con-meno-salute-un-allarme-epidemiologico/
Folgheraiter, F. (2011). Fondamenti di metodologia relazionale: La logica sociale dell’aiuto. Erickson.
Folgheraiter, F. (2014). Non fare agli altri. Il benessere in una società meno ingiusta. Erickson.
Folgheraiter, F. (2022). C’è rispetto e Rispetto: Riflessioni su «dignità» e «reciprocità» nel Lavoro socio-assistenziale con gli anziani. Note in margine al Convegno «Anziani: dignità, relazioni, cure» rivolto ai Dirigenti e agli operatori professionali dei Servizi di aiuto alla persona (Trento, Erickson, ottobre 2022, testo non pubblicato).
Folgheriter, F. (2024). Relational Theory in Social Work: Phenomenological Foundations, Cognella Academic Publishing.
Fook, J. (2016). Social work: A critical approach to practice. SAGE.
Fosti, G., Notarnicola, E., & Perobelli, E. (2024). La sostenibilità del settore Long Term Care nel medio-lungo periodo — 6° Rapporto Osservatorio Long Term Care. EGEA.
Kitwood, T. M. (1997). Dementia reconsidered: The person comes first. Open University Press.
Krumer-Nevo, M. (2020). Radical hope: Poverty-aware practice for social work. Policy Press.
Lucatoni, D., & Principi, A. (2022). Politiche per l’invecchiamento attivo in Italia: Quali possibili obiettivi nelle Regioni, nelle Province Autonome, nei Ministeri e nei Dipartimenti presso la Presidenza del Consiglio dei Ministri? Raccolta di rapporti. https://famiglia.governo.it/media/2704/possibili-obiettivi-politiche-per-linvecchiamento-attivo-in-italia-raccolta-dei-rapporti.pdf
MIGEP — Federazione nazionale delle professioni sanitarie e sociosanitarie (2022). Carta Etica dell’OSS. https://www.migep.it/app-data/home/620c3cb0-4ca8-4df4-b185-d5eb0a6de9aa/carta-etica-10-02-2022.pdf
Rossi, G. (1989). Figli adulti e genitori anziani: Qualità della relazione e sentimento di obbligo. In E. Scabini, & P. Donati (Eds.), Vivere da adulti con i genitori anziani. Vita e Pensiero.
Sevenhuijsen, S. (2003). Citizenship and the ethics of care: Feminist considerations on justice, morality and politics. Routledge.
Strier, R., & Binyamin, S. (2014). Introducing anti-oppressive social work practices in public services: Rhetoric to practice. The British Journal of Social Work, 44(8), 2095-2112.
Thompson, N. (2021). Anti-discriminatory practice: Equality, diversity and social justice. Red Globe Press-Macmillan.
Weiss, I., Gal, J., Cnaan, R. A., & Maglajlic, R. (2002). Where does it begin? A comparative perspective on the professional preferences of first-year social work students. British Journal of Social Work, 32(5), 589-608.
World Health Organization — WHO (2021). Global report on ageism. https://apps.who.int/iris/bitstream/handle/10665/340208/9789240016866-eng.pdf
Folgheraiter, F. & Raineri, M. L. (2025). The Relationship with the Suffering Other. An Analysis of Attitudes Towards Respect for Older People in the Context of Social Services. Relational Social Work, 9(1), 3-25, doi: 10.14605/RSW912501.

Relational Social Work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License
-
1 For example: «The social worker... acknowledges the value, intrinsic dignity, and uniqueness of every individual» and «The social worker strives to ensure that professional intervention takes place under conditions and within timeframes that safeguard the dignity, protection, and rights of the person» (Articles 5 and 19, Code of Ethics of Social Workers, CNOAS, 2020). «The Professional Educator... must respect the personality and dignity of service users; the educator is required to ensure, in the exercise of their duties, that the conditions are in place to guarantee respect for the individual’s personality and human dignity» (Articles 1 and 4, Code of Ethics of Professional Educators, ANEP, 2015). «Professionals must carry out their practice with the aim of upholding respect for the human person...»; «Each individual worker must contribute to ensuring that patients are able to experience their stay in care and their health vulnerability with calm and dignity» (Articles 1.5 and 6.4, Ethical Charter of Social and Health Care Workers, MIGEP — National Federation of Health and Social Health Professions, 2022).
-
2 Art. 26 Code of Ethics for Italian Social Workers, CNOAS, 2020.
-
3 Art. 11 Code of Ethics for Italian Social Workers, CNOAS, 2020.
-
4 Art. 1, paragraph 1, L. 328/2000.
-
5 For a broad collection of examples: Lucatoni &Principi (2022), Politiche per l’invecchiamento attivo in Italia. Presidenza del Consiglio dei Ministri, Dipartimento per le politiche della famiglia.